The correct diagnosis is sinus rhythm with premature ventricular contractions and ventricular parasystole (Figure 2).
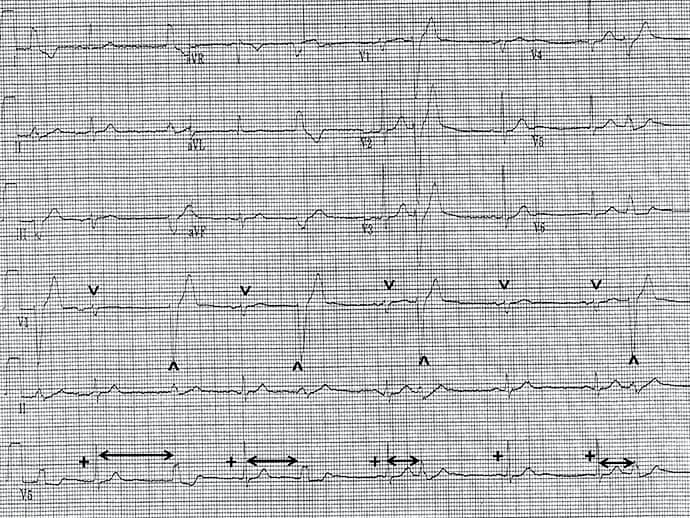
Figure 2. Courtesy of Philip J. Podrid, MD.
Discussion
The rhythm is irregular. There are narrow (˅) and wide complexes (^). The narrow QRS complexes are preceded by a P wave (+) with a stable PR interval (0.20 sec). The P waves are positive in leads I, II, aVF, and V4-V6. These are sinus complexes.
Two sequential sinus complexes occur (complexes 8-9) and the rate is 50 beats/min. The narrow sinus QRS complexes have a normal duration and morphology with a tall R wave in lead V2, which is termed early transition and is due to counterclockwise rotation in the horizontal axis; imagine the heart viewed from under the diaphragm. With counterclockwise rotation, left ventricular forces develop earlier and are seen in the right precordial leads. The axis is leftward (physiologic) between 0° and -30° (positive QRS complex in leads I and II and negative in lead aVF). The QT/QTc intervals are normal (440/400 msec).
A wide QRS complex (0.14 sec) (^) follows most of the sinus complexes; it has a different morphology and is not preceded by a P wave. These are premature ventricular complexes. They all have the same morphology and therefore are unifocal. However, there are variable coupling intervals (↔), known as the interval between the sinus complex and the premature ventricular complex.
Therefore, the mechanism for the premature ventricular complexes is not reentry, which is the most common mechanism for ventricular arrhythmia. With reentry, the impulse circulates around a fixed circuit and there is a fixed (constant) coupling interval between the premature complex and the preceding sinus QRS complex. When the coupling interval is variable, the mechanism for the premature ventricular complex is an ectopic focus, termed ventricular parasystole. The variable coupling interval is caused by an entrance block into the focus (the focus is not suppressed and continues to generate an impulse at its own rate), and there is also exit block from the focus (activating the ventricular myocardium only when the myocardium is not refractory and can respond).
Philip Podrid, MD, is an electrophysiologist, a professor of medicine and pharmacology at Boston University School of Medicine, and a lecturer in medicine at Harvard Medical School. Although retired from clinical practice, he continues to teach clinical cardiology and especially ECGs to medical students, house staff, and cardiology fellows at many major teaching hospitals in Massachusetts. In his limited free time he enjoys photography, music, and reading.
Follow Medscape on Facebook, X (formerly known as Twitter), Instagram, and YouTube
Medscape Cardiology © 2023 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: ECG Challenge: Is Heart Disease Causing This Man's Irregular Pulse? - Medscape - Dec 22, 2023.









Comments