This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I'm Dr Matthew Watto, here with Dr Paul Nelson Williams. We're going to be recapping some of our favorite pearls on hematuria, which is a really common problem. Gross hematuria — should we worry about it?
Paul N. Williams, MD: We talk about it in the podcast Hematuria with Dr Derek Fine. You mentioned that microscopic hematuria is seen often in primary care. We will get a urinalysis for whatever reason, and it comes back with microscopic hematuria. That's a different situation from the patient who comes in with gross hematuria, meaning, visible blood in their urine. By definition, gross hematuria is a higher-risk condition. And when we're talking about risk, what we worry about specifically is malignancy, first and foremost. Gross hematuria immediately puts the patient in a high-risk category that warrants workup. Clots, if present, are all the more urgent and suggest that this might be a urologic cause as opposed to a glomerular cause.
Original image available to view here.
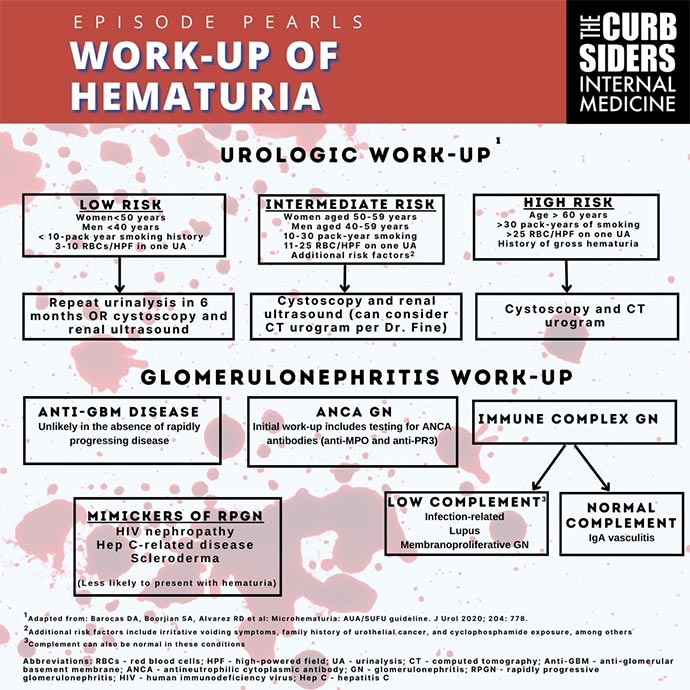
Watto: We also talked about the risk factors for malignancy. They are fairly intuitive: older age and smoking history (especially more than 30 pack-years). The age cutoff is 60 for the highest-risk category. Gross hematuria or even microscopic blood more than 25 red blood cells per high-power field puts them in that high-risk category also.
Now, Paul, if my patient is on warfarin, I'm not worried. I know why they're bleeding — they're on warfarin!
Williams: Or a DOAC [direct-acting oral anticoagulant]. It's a great point, but anticoagulants don't excuse you from working up hematuria. If you look at the literature, a patient who is on anticoagulants and has hematuria tends to have better outcomes, probably because the anticoagulation actually caused them to declare themselves earlier than they otherwise would have. So warfarin just kind of makes something that's already there more apparent. It's a fun fact — one of the few times you feel good about bleeding with warfarin. But patients on anticoagulation with hematuria are owed the same workup as anyone else with hematuria.
Watto: So we have our urologic causes of bleeding. That could be something in the bladder, the prostate, or somewhere in the urinary tract. How are we going to work up those urologic causes? What sort of testing would you recommend?
Williams: It kind of depends on the patient in front of you. Most patients are going to warrant some imaging. If the patient is at low-moderate risk, you may be able to get away with doing an ultrasound. Dr Fine said ultrasound might pick up things like renal cysts or other large structural causes. But patients about whom you have a real concern — for example, gross hematuria — are probably going to need CT urogram and cystoscopy. And obviously, we'll just be facilitating that with the urologist. But I think once you're in that high-risk category, whether it's by age or presence of gross hematuria or prolonged tobacco exposure, CT urogram or cystoscopy is where you're going to go in most cases.
Watto: I'm doing the same with my patients. If they're older or if I'm more worried about malignancy because of their smoking history, I am more likely to get the CT urogram with contrast and refer them first to cystoscopy than to renal ultrasound if they are 40 years old and never smoked, or have maybe 4 RBCs of microscopic blood. Maybe then I'll get a renal ultrasound. I'm not as worried. But I still watch those people closely.
Now, Paul, when should we send the patient to our friendly neighborhood nephrologist?
Williams: I always just assume that nephrologists are smarter than me, so almost any reason you can send a patient to one is a good idea. But if you're worried about glomerular bleeding specifically — or let me put that a different way: Things that would prompt you to worry about glomerular bleeding would be any degree of albuminuria (that should make you a little bit nervous), rapidly increasing blood pressure from their baseline (that should make you very nervous), or if they have rising creatinine levels. You don't necessarily see those things with all kinds of glomerular bleeding, but they do suggest etiologies that are worrisome and need more urgent intervention.
So if you see those things, the source of bleeding is more likely to be nephrologic, and the patient needs to see a nephrologist. This is a patient for whom you make a phone call; this isn't someone who gets a 3-month follow-up appointment. You need to get them seen quickly.
Watto: To hear the full podcast, which I highly recommend, click here.
Follow Medscape on Facebook, X (formerly known as Twitter), Instagram, and YouTube
Credits:
Image: The Curbsiders
© 2023 WebMD, LLC
Cite this: Matthew F. Watto, Paul N. Williams. Hematuria: When to Worry About Bloody Urine - Medscape - Nov 06, 2023.








Comments