Anyone who has learned to read ECGs has heard it before: "You can't diagnose acute myocardial infarction (AMI) on an ECG in the presence of a pacemaker." We have actually heard the same dictum regarding the diagnosis of AMI on ECG in patients with left bundle branch block (LBBB).
In 1996, Sgarbossa and colleagues published a set of ECG findings that could be used to diagnose AMI in the presence of LBBB with high specificity. These Sgarbossa criteria were later refined and validated as the modified Sgarbossa criteria, which have been widely discussed and accepted by many as a reliable means of diagnosing acute coronary occlusion in the presence of LBBB. Criteria for diagnosing acute coronary occlusion in the presence of a ventricular pacemaker were also suggested by Sgarbossa and colleagues in 1996, but these criteria had a tougher time gaining acceptance because the original study population was so small and high-quality validation studies were lacking.
However, Dodd and colleagues have recently published a high-quality trial that validated the use of the modified Sgarbossa criteria for diagnosing acute coronary occlusion in the presence of a ventricular paced rhythm. They performed a retrospective case-control study involving 16 cardiac referral centers in the United States and four other countries and included adult patients with ventricular paced rhythms presenting with symptoms of acute coronary syndrome between January 2008 and January 2018.
The main study group involved patients who were diagnosed with occlusion myocardial infarction (OMI), defined angiographically as thrombolysis in myocardial infarction grade 0-1 flow or angiographic evidence of coronary thrombosis and peak cardiac troponin I ≥ 10.0 ng/mL or troponin T ≥ 1.0 ng/mL. These patients were compared with two control groups: Control group 1 included non-OMI patients who underwent coronary angiography for presumed type I AMI but did not meet the definition of OMI; group 2 consisted of randomly selected emergency department patients with ventricular pacers presenting with symptoms concerning for acute coronary syndrome but who were ruled out for OMI. This second group did not undergo angiography. Researchers evaluated the presence or absence of the modified Sgarbossa criteria on the ECGs.
The modified Sgarbossa criteria on ECG consisted of any of the following:
A. Concordant ST-segment elevation of > 1 mm in any lead (Figure 1).
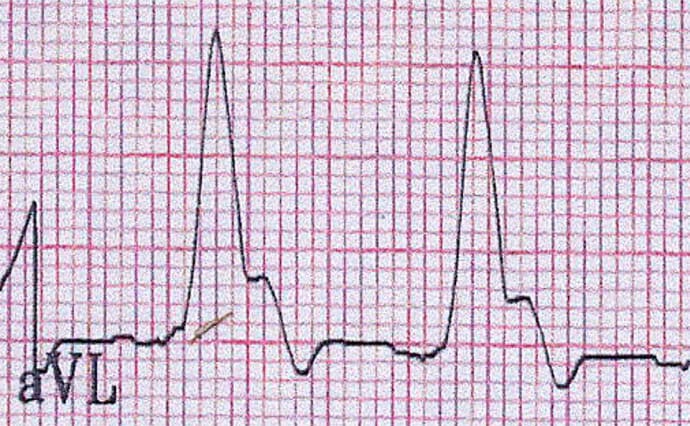
Figure 1.
B. Concordant ST-segment depression of > 1 mm in any of leads V1-V6 (Figure 2).

Figure 2.
C. Discordant ST-segment elevation with ST/S ratio > 25% in any lead (Figure 3).

Figure 3.
STE = ST-segment elevation
The researchers identified 59 patients who met the definition of OMI: 90 patients in the first control group and 102 patients in the second control group. The researchers found that the sensitivity of the modified Sgarbossa criteria for diagnosing OMI was 86% (far superior to the original Sgarbossa criteria's sensitivity, which was found to be 56%). These modified criteria had good specificity as well: When the modified criteria were applied to the first control group, the specificity was 84%; when applied to the second control group, the specificity was 96%.
In Summary
Patients with ventricular pacers typically have many of the same risk factors and comorbidities that increase their risk for AMI. As the indications for ventricular pacing increase, the number of patients presenting to emergency departments with pacers are rising; so too are the number of patients with AMI. When AMI is due to an acute coronary occlusion, immediate acute reperfusion therapy (fibrinolytics or percutaneous coronary angiography) is considered the optimal management. The early decision to provide this therapy hinges on ECG interpretation.
The work of Dodd and colleagues has provided us with a significant advance in electrocardiography, dispelling decades of teaching to all-but-ignore the ECG in patients with ventricular pacers presenting with symptoms of acute coronary syndrome. We all owe it to our patients to both learn the modified Sgarbossa criteria and apply them in the emergency department when patients with ventricular pacers present with symptoms concerning for acute coronary syndrome.
Amal Mattu, MD, is a professor, vice chair of education, and co-director of the emergency cardiology fellowship in the Department of Emergency Medicine at the University of Maryland School of Medicine in Baltimore.
Follow Dr Mattu on Twitter.
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
Credits:
Lead image: Dreamstime
Figure 1: Amal Mattu, MD
Figure 2: Amal Mattu, MD
Figure 3: Amal Mattu, MD
Medscape Emergency Medicine © 2021 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: Amal Mattu. Diagnosing Acute Coronary Occlusion in a Paced Patient: Busting a Myth - Medscape - Nov 18, 2021.










Comments