Eric J. Topol, MD: Hello. I'm Eric Topol, editor-in-chief of Medscape. It's a real delight to welcome John Rogers from Northwestern University in Evanston, Illinois. John is probably the world leader in developing creative sensors that interact with the human body. Welcome, John.
John A. Rogers, PhD: It is a pleasure to be here.
Dr Topol: You went to the University of Texas at Austin, and then on to the Massachusetts Institute of Technology (MIT), right?
Dr Rogers: Yes. I was at MIT for 6 years. I got master's degrees in physics and chemistry, and then a PhD in physical chemistry. After that, I got a junior fellowship at the Harvard University Society of Fellows, which was like a super-post-doc, a 3-year position. The appeal was that it provided a salary and a stipend, and you could sort of do whatever you wanted.
I ended up splitting my time between work in the Harvard laboratory of George Whitesides, a famous materials chemist and entrepreneur, with the other half spent with a start-up company that we launched out of MIT based on my PhD research. That was a really fun time, from 1995 through 1997.
Dr Topol: Then you went to Bell Labs?
Dr Rogers: Yes. I interviewed for a number of positions, but I was always drawn to the interface between science and technology. Bell Labs in those days was like the New York Yankees of science, with its focus on materials, technology, lasers, and integrated circuits. I spent 5 great years there, during which I was really able to expand my areas of expertise.
That "Bell Labs–ian" mindset has really stayed with me and shaped my research. After Bell Labs, I went to the University of Illinois at Urbana.
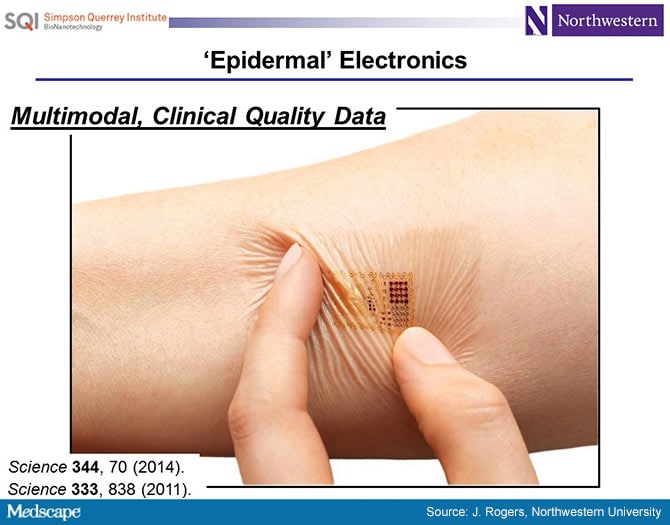
'Epidermal Electronics': Thin Skin Sensors
Dr Topol: I first learned of you from a 2011 paper in Science[1] about "skin chips," which you pioneered. Tell us a bit about that.
Dr Rogers: That was a really important paper for us. My core expertise is in electronic materials. Most people who are doing academic research in electronic materials are thinking about a future of electronics driven by Moore's Law.
Transistors are getting smaller and smaller; microprocessors have more and more transistors per unit area, at higher and higher clock speeds, with more and more sophistication in their operation. That is a really compelling area for research, because to enable a continuation of Moore's Law will require a lot of scientific discovery and new academic insights into materials at those scales.
We have been interested in a different future of electronics, not so much driven by the critical dimensions of transistors, but thinking about electronics as a possible interface to the human body. Here, you need to consider things around materials biocompatibility and, maybe more important, physical properties that enable an intimate integration of circuit technology with the soft-textured, time-dynamic surfaces that you find in biology. It's quite a bit different from anything that has ever been present in commercial forms of integrated circuits, which were all built in the rigid planar surfaces of semiconductor wafers.
This paper was the first demonstration of all the key ideas around the material science, the mechanics' designs, the device architectures, the system-level considerations that allowed us to create skin-like forms of electronics.
Dr Topol: I remember the pictures from the Science paper, with these little skin chips on the forehead for an electroencephalogram and on the chest for a cardiogram, and thinking that this was mind-blowing.
What I do not understand is how you moved from this engineering background with chemistry and physics into wanting to deal with the body and coalescing chips with it.
Dr Rogers: It's an interesting story. We got into this whole area of flexible electronics when I was back at Bell Laboratories, where we were developing new classes of semiconductor materials. The idea was that if you could create integrated circuits on sheets of plastic, you might be able to build new classes of consumer gadgets. In particular, we were interested in paper-like flexible displays.
I was giving a talk in electrical engineering at the University of Pennsylvania on this topic and some neuroscientists came up to me afterwards. They said, "Hey, these are cool for large-area steerable antennas for the military or flexible displays for consumer applications, but have you ever thought about putting these things on the brain? That would be really interesting, because you could map electrical activity on the brain."
I had never really thought about that bio interface until that time, and it struck me as a huge opportunity. So, we started collaborations on that basis. We were also interacting with cardiologists from the University of Pennsylvania Medical School. Understanding epilepsy also turned out to be an area of focus, using these sheets as diagnostic platforms.
This was a direction I wanted to pursue, but as you know, it's ultimately the students who have a large impact on your research. And this was such a compelling idea for them. They saw a much greater and higher purpose in working on technologies that could have a positive impact on human healthcare than technologies that could be used for a new consumer electronics gadget. So it was those two things that came together.
Dr Topol: The things you previously developed were already mind-blowing, but since then, you've developed the Snapchat of chips in the body.
Dr Rogers: I have never heard it referred to that way! (laughing) That's pretty good!
Dr Topol: It disintegrates, dissolves, and self-destructs. It's incredible! Then you had all of these other ideas to use these chips on the brain and in the heart, catheters with chips, testing for things like hydration or blood pressure. Is there anything you cannot measure with these chips?
Dr Rogers: That is a good question. Most of the sensors that we focused on up to this point have really emphasized physical property measurements, such as strains, stresses, electrical potential, temperature, and things like that. I think the frontier is in biochemical rather than biophysical measurements.
Sweat: The 'Holy Grail'
Dr Topol: You published a Science Translational Medicine article[2] that featured this very cool design for a sweat sensor that can measure lactate and electrolytes, which obviously was a stunner as well, but where can that go? Do you have to have actual sweat or can you just get that right on the skin?
Dr Rogers: Right now, we are just capturing sweat that is emerging from the skin in physical liquid form. The eccrine glands are acting as pumps to push that sweat into these microfluidic analysis networks. We can do a lot with that once we have even just microliter volumes of sweat; we can route it around and do all kinds of analysis.
But, as you know, your body is constantly undergoing sweating without enough liquid volume to form well-defined droplets, and that evaporates almost immediately. We think there is a great opportunity for new device designs and materials that can capture that insensible sweat, so you do not have to be physically exercising in order to capture this kind of bio fluid. That's an area of ongoing research for us and it's tantalizing.
Dr Topol: Do you think you'll be able to do it?
Dr Rogers: It seems like it should be possible. If you look at your skin under a microscope, you can see that your sweat glands are constantly firing. There is liquid there, but it immediately evaporates. Right now we can capture the water vapor associated with insensible sweat and condense it in our devices. So we thought we had the problem solved, but unfortunately the evaporation process leaves all the biomarkers behind.
Dr Topol: If you can do that, it will be like the Holy Grail, as all of these things correlate so well with what is in the blood. That will be a big one.
You just moved to Northwestern University a year ago, and what I learned just today is that you have taken these chips, which are no longer just fascinating breakthroughs but are now in infants, in kids, in intensive care units. Tell us about that.
Dr Rogers: That was one of the primary motivations in moving from the University of Illinois, where I spent 13 very productive years with great colleagues. However, there is no medical school in Urbana.
We had been doing pretty well collaborating with medical schools at different universities, in St. Louis, continuing our work with the University of Pennsylvania Medical School, and so on. But we perceived greater opportunities being geographically co-located with an active medical school with researchers there.
The move to Northwestern has really blown out the number of interactions we have with clinicians. It's great to publish papers and educate the graduate students and so on, but we are defining success by proliferation of the technologies. The best, most effective way to do that is to get engaged very intimately with a medical school.
We have all kinds of human subject studies underway. As you mentioned, we have devices in the NICU, the PICU, the ICU. We also have a number of engagements with the Rehabilitation Institute of Chicago, which is now called the Shirley Ryan AbilityLab. There are tremendous opportunities there with Parkinson's patients, patients undergoing rehab from stroke. We are studying aphasia, dysphagia, all kinds of stuff. Our bandwidth is really just limited by the numbers of students that we have in the group.
Dr Topol: It's so striking to compare a picture of a newborn attached to all of these wires everywhere on their body, with a picture of a newborn with just two of your skin chips on their chest and foot. It feels like this is a whole new world. These are the sorts of developments that will make ICUs and hospitals unrecognizable using this kind of monitoring, right?
Dr Rogers: We hope so. That is what we are aiming for. I think that NICU example is a pretty compelling one, where the skin-like-form factor is absolutely essential, not just a convenience.
Dr Topol: When you take [the old wire monitors] off, you dehisce the skin in infants, particularly sick ones. The idea that you can do this in the way that you have invented is just remarkable. In addition, you are able to collect data that you could not even get from the old systems.
Dr Rogers: That is really the frontier. Right now, we are focusing on reproducing the clinical tools that are used today but making the devices much less invasive. But once you have a foothold, once you have reproduced what is being done now, there will be the ability to extend beyond that and do all kinds of measurements that are not even possible right now.
For example, we can measure cardiac auscultation, which is not done in the NICU today. We can also measure pulse arrival times and obtain continuous blood pressure measurements, which are also not done today. There are all kinds of opportunities. That is where we are looking in terms of the future research opportunities.
Funding Challenges
Dr Topol: You touched on the fact that when you went to Northwestern it gave you a much better opportunity to liaise with the medical community directly, not just through remote collaborations. What is holding back this engineering-medicine coalescence? We need it to advance the field, and you are the exemplar. Why do you think it doesn't happen more often?
Dr Rogers: It's hard for me to say exactly. I can say from my own personal experience that it is the translational engineering parts that tend to be difficult to do in an academic setting. There are relatively few funding streams that allow you to take what is developed, foundational science from an academic setting and move it into meaningful human deployments in a clinical trial.
We have had the good fortune that there has been engagement at the philanthropic level to help us try to solve that problem, but that is not a scalable model to get a larger fraction of the engineering community engaged in this kind of thing.
I think there are opportunities for foundations, or maybe the federal funding agencies, to look and think about whether it is useful to place bets on that style of research. It is not fundamental science discovery, but it is an important piece because in order to get things out of the lab, you have to do these things, right? I think the results of that kind of work provide deep and important insights into guiding the scientific questions in the basic research.
It is an important piece, and absent funding specifically for that, it means you have to look for philanthropy, you have to start up companies and raise venture capital resources. It's time-consuming, slow, and not particularly efficient. There is that aspect of the funding landscape that could really accelerate a lot of the work in this space.
Working Under the Media's Microscope
Dr Topol: One of the things that I found interesting about you was that you are one of the few engineers to have ever had a profile in The New Yorker, "The Body Electric,"[3] which ran in 2013. Tell us what it was like to hang out with a New Yorker journalist and have them embedded with you in your lab.
Dr Rogers: It was interesting. It was a great experience. It was a little nerve-racking, to be honest with you, because she spent two full days with me, morning to night, shadowing me as I went about my business. She was trying to collect as much information as she possibly could to write the piece. I put a fair amount of thought and advanced preparation into that, so that the meetings were such that she was able to get the insights she needed to write the article. But you never know how those things are going to turn out.
Dr Topol: It was a stunner.
Dr Rogers: It turned out pretty well. I was a little bit nervous. I didn't even read it myself until several months later. I did not want to look at it, but a lot of people have seen it. It has been an amazing thing.
Dr Topol: I hope the Medscape community will take the time to read it, because it really tells a lot about you. It doesn't even mention all of the things that you have been recognized for, like the MacArthur Fellowship (aka "the Genius Grant"), the Lemelson-MIT Prize, the Smithsonian Ingenuity Award, and your election to the National Academy of Engineering, of course.
But you have been rocking. You have been changing the field. There are not so many pioneers that have taken engineering to medicine as you have, in a very distinct way.
Shining a Light on Optogenetics
Dr Topol: The other area that is, of course, a hot one right now is optogenetics. I would not be surprised if you are well into that, too. Is that right?
Dr Rogers: We are pretty deep into that, yes. We had a paper in 2013 in Science[4] where we leveraged our ability to make very tiny, very thin semiconductor devices. That is kind of foundational for the skin-integrated devices, which is a lot of what we do, but those same ideas apply to light-emitting diodes (LEDs).
The conventional way to do optogenetic studies, at least of rodent animal models, is to use fiber-optic cables developed by the telecommunication industry to deliver light to targeted regions of the deep brain. That sort of works. The problem is that it physically tethers the animal to an external light source, which impacts their natural behavior patterns. That, in turn, prevents the study of social interactions, because two animals with fiber-optic tethers immediately get tangled up with one another.
We began to think about whether we could take these very tiny LEDs and just inject them directly into the brain, get rid of the external light source and the fiber-optic cable, and wirelessly deliver power to the LEDs down in the region of interest in the brain, and do optogenetics in that way.
It turned out to work. It is amazing that you can do the thermal management at such a level that you don't damage the neurons that you are trying to stimulate with the light, and it becomes enabling.
There is really a lot of interest in access to the technology. We actually started a small company around that technology and we now have around 30 systems worldwide. Basically, this is a radiofrequency control box with software interface, and the tiny implants provide an ability to inject LEDs down into the deep regions of the brain. The wireless harvester sits subdermally. The mice with these LEDs in their brains look exactly like mice that have not been modified in that way.
Dr Topol: It has some scary potential. You can imagine it as a replacement for deep brain stimulation, almost like a pacemaker for the brain. Of course, as a research tool, it is quite remarkable.
Looking Ahead
Dr Topol: As you go forward, what other areas do you see for their challenges, but also for their big potential?
Dr Rogers: We are excited about transient electronics, which you referred to a few minutes ago. The notion of a medicine that is engineered around electronics that dissolve in the body is pretty attractive.
As an example, we have active programs in electrical stimulators that interface with damaged peripheral nerves and completely implant into the body. You can then wirelessly deliver electrical pulses to the nerve to accelerate neuroregeneration and healing. In that context, you would like a device that is ultimately bioresorbable, because you do not need the device around once the nerve has healed.
That kind of system, perhaps coupled to a sensing modality that allows a closed feedback–loop-type operation, is something that we think has an important future. We have a lot of research efforts in that direction.
Dr Topol: It is clear that you are moving beyond the sensing capability to the actual treatment. It's pretty formidable.
Dr Rogers: Thank you.
Medscape © 2018 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: The Future of Medicine From a Leader in Biosensors - Medscape - Mar 15, 2018.







Comments